
Types of bone irregularities after FFS Surgery

In this series of informative articles that Facialteam publishes periodically, we want to create an educational tool for patients based on our experience, accumulated over more than ten years working in the field of facial feminization surgery and facial gender confirmation surgery. Our idea is to provide clear, honest and objective information that is useful for patients, whether they have already received treatment or are in the process of looking for a surgeon. The contents of these publications are based on our own daily clinical practice and on the information gathered from more than 1,500 patients operated on by our facial feminization group.
One common source of questions and concerns for some patients is the presence of depressions or irregularities after surgical forehead treatment. We are going to explain some of the reasons for these depressions and irregularities and possible solutions to treat or camouflage them.
It’s important to understand that the characteristics of each individual patient determine the visibility and scope of this problem. This is due to the fact that the anatomy of the forehead can vary greatly from patient to patient. Very fine skin with little fat and/or muscle content is more likely to have small, possibly visible bone irregularities. On the contrary, patients whose foreheads have fattier skin and a thicker adipose panicle or muscle volume can better conceal and soften possible irregularities on the bone plane.
What causes forehead depressions or irregularities?
The main cause of the appearance of these irregularities is the phenomenon of bone resorption. Bone resorption is the partial loss of bone in a specific area. If the bone loss is significant, it may be visible or palpable through the skin. There are other reasons this occurs too, such as the use of fillers, the type of instrument, poor technique, failure to fix bone fragments, and alterations in the muscle or other tissue, for example.
When does bone resorption occur and why?
The forehead bone is made up of two layers or two different types of bone: cortical bone and medullary or spongy bone. The cortical bone is the outermost bone layer, the one in contact with the soft tissues (muscle, fat, skin). This bone is compact and very hard, with very few blood vessels and a thickness that can vary from 2 to 10 mm. Generally speaking, the cortical bone does not have a tendency to reabsorb (disappear) and it is the bone on which bone burring is most often done. Under the cortical bone layer (which acts as a protective layer) is the medullary or spongy bone. This is a porous bone, similar to a sea sponge –hence, the name– with a large number of interior blood vessels and a softer and more fragile consistency than the cortical bone. This medullary bone is more likely to reabsorb if it becomes exposed (in other words, if it doesn’t have the cortical bone layer to protect it).
At times, during bone burring surgery (which, as noted above, is usually done on the cortical bone), the medullary bone becomes exposed. If this exposure is limited and doesn’t affect a large surface area, the possibility of resorption (bone disappearance) is low, since this medullary bone undergoes a phenomenon known as corticalization, meaning that it becomes harder (like the cortical bone) during the healing period. If the exposed medullary bone area is large, there is a higher possibility of resorption. This resorption phenomenon occurs during the first weeks or months after surgery. If the size of this resorption is large, it may become visible through the skin later, appearing as a depression, cleft or irregularity of variable size.
Are there any other mechanisms that might cause bone resorption?
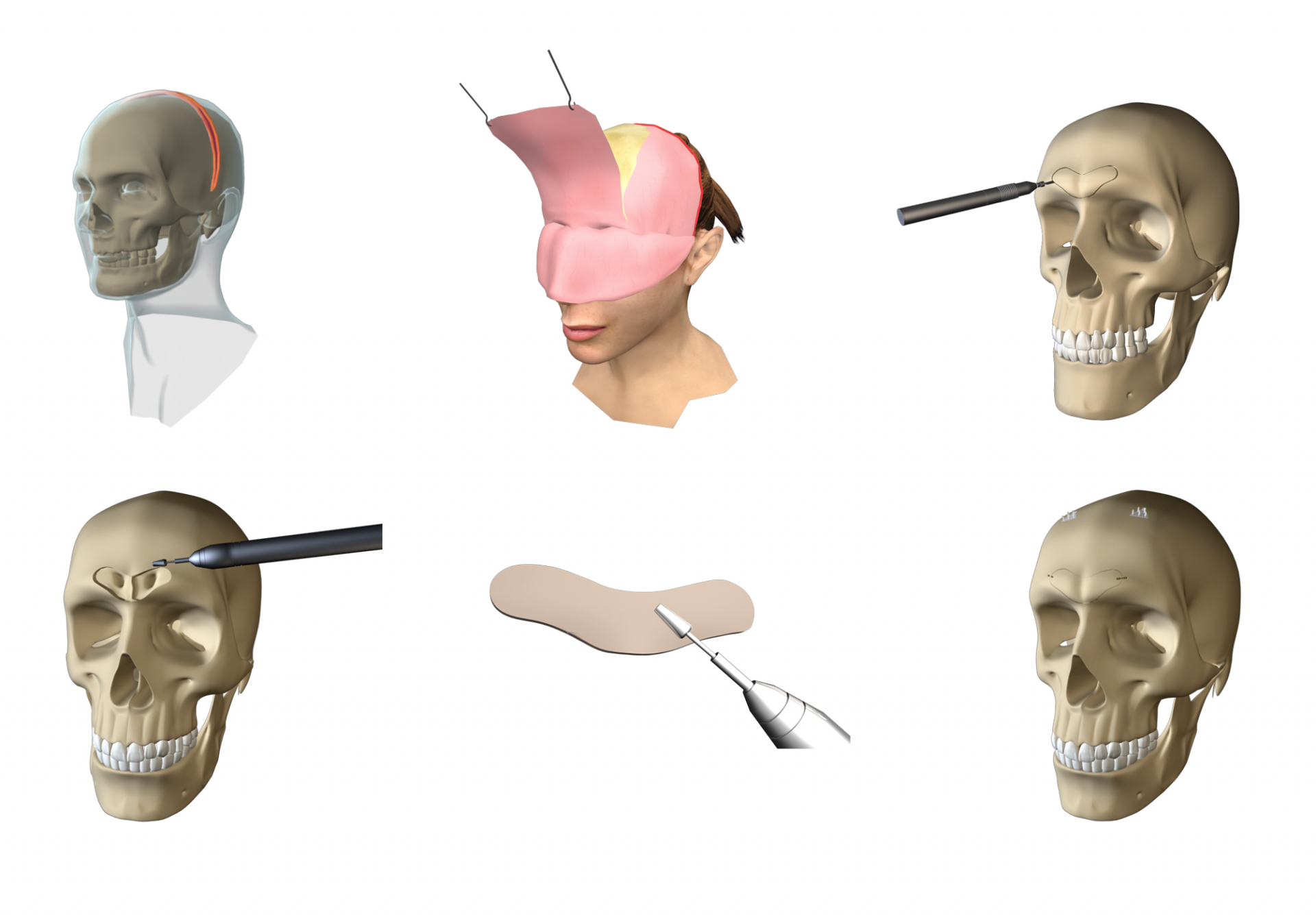
In most cases, forehead reconstruction surgery involves the frontal sinus region. At this time, according to the technique of choice of each specialist, different types of procedures are used to work in the sinus region. With a very high percentage of patients, the anterior wall of the sinus is removed and later fixed, which in practice involves cutting the bone, removing a bone fragment and repositioning this fragment. See a study published here. (Fig. 1). This fragment must be fixed as stably as possible to guarantee bone healing and the proper regeneration of the surgical area. If the fixation system or material used with this bone does not guarantee adequate stability, micro-movements during the bone healing phase may trigger poor bone consolidation, resulting in resorption or disappearance of the bone at that level.
Another possible reason for bone resorption is associated with the presence of overly weakened bone in the sinus region. At times, after reconstructing and burring the sinus area, very weakened or even perforated areas may remain. According to the size of these areas, resorption may occur as a result. This can also happen when the surgeon burrs the frontal sinus wall directly, instead of a doing the reconstruction on the sinus, and perforates or excessively weakens it.
Other reasons bone irregularities occur
In addition to bone resorption, another set of situations may produce irregularities, asymmetries or depressions, as we explain below.
- Poor burring technique. The aim of forehead burring or bone recontouring is to harmonize and soften this region. If the recontouring is not done correctly or using the required tools, it may produce irregular or asymmetrical areas that are later visible or palpable through the skin.
- The use of filler materials. At times, while working on the forehead, some specialists use different heterologous (not coming from the patient) materials (cement, protheses, implants made of different materials, etc.). The aim can be to increase the volume in a specific area, obtain a rounded format or conceal frontal bossing by filling less protected areas. Regardless of whether these procedures guarantee optimal and/or satisfactory results, these materials can occasionally produce asymmetries, irregularities, unharmonious contours or migrations of the material to undesired areas, with a consequent unaesthetic result for the patient.
- Alterations of the forehead muscle. After surgery and soft tissue repositioning, the frontal musculature may undergo different types of phenomena: less contraction capacity, loss of volume, a more obvious middle line, etc. These phenomena may appear as asymmetries or irregularities of the forehead contour.
Treatment alternatives for bone irregularities
Having listed the different situations that may produce some type of asymmetry, depression or irregularity after forehead recontouring surgery, what follows are the different treatment alternatives for each case.
- Small or limited irregularities or depressions. This group includes all the irregularities that are only slightly visible or palpable and are not problematic for the patient, except for the associated aesthetic problem. These should be approached conservatively and with minimal invasion. One of the possible solutions is to conceal or camouflage the problem area with a filler material like fat or hyaluronic acid, avoiding the need for another surgery.
- Depressions that are extensive or in highly visible areas. These irregularities are extremely aesthetically problematic for the patient. The ideal solution is to reconstruct the problem area. This involves another surgical session and the possibility of using different types of material that vary according to the type of defect and its location, such as titanium mesh of different thicknesses and sizes, bone grafts, etc.
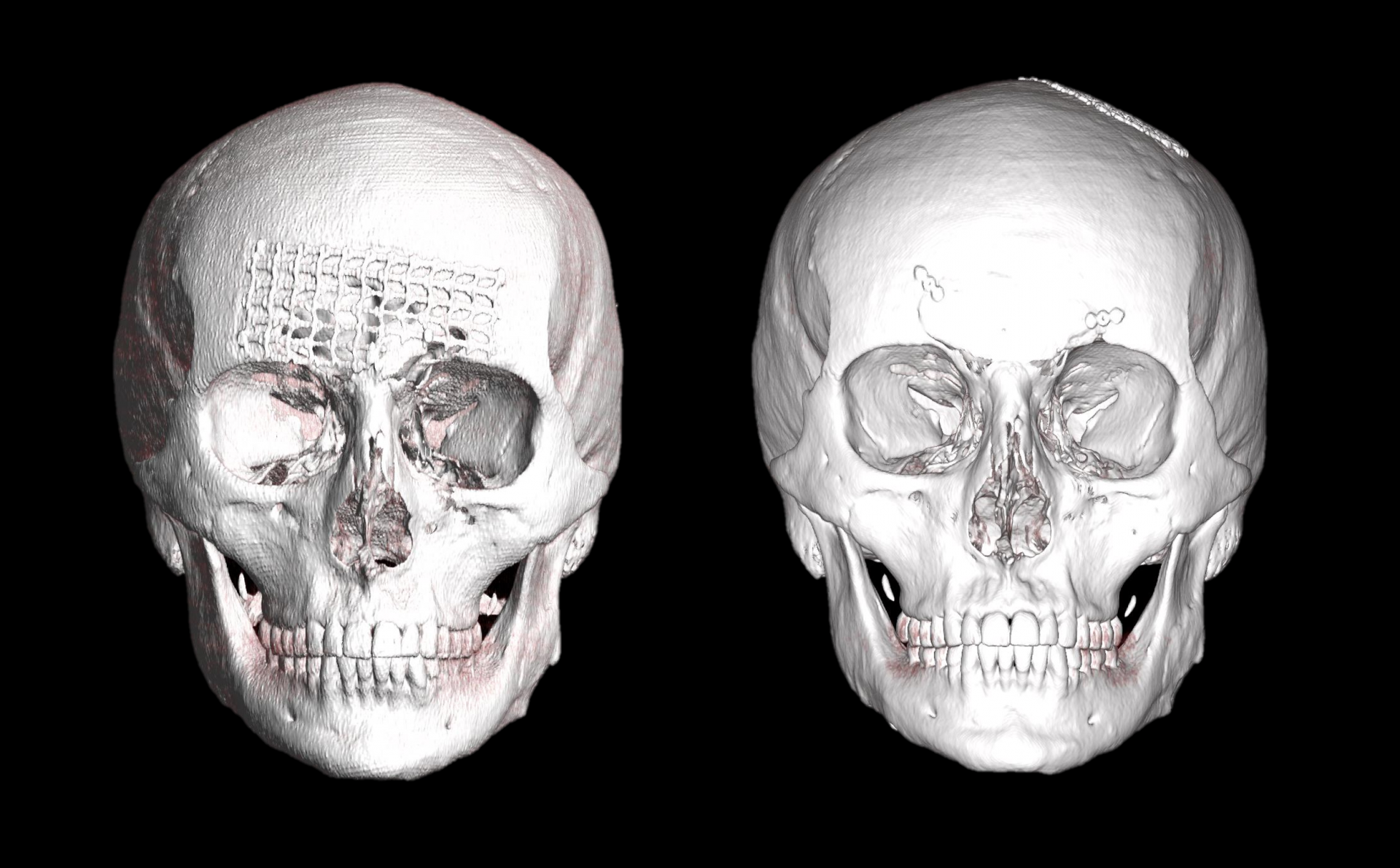
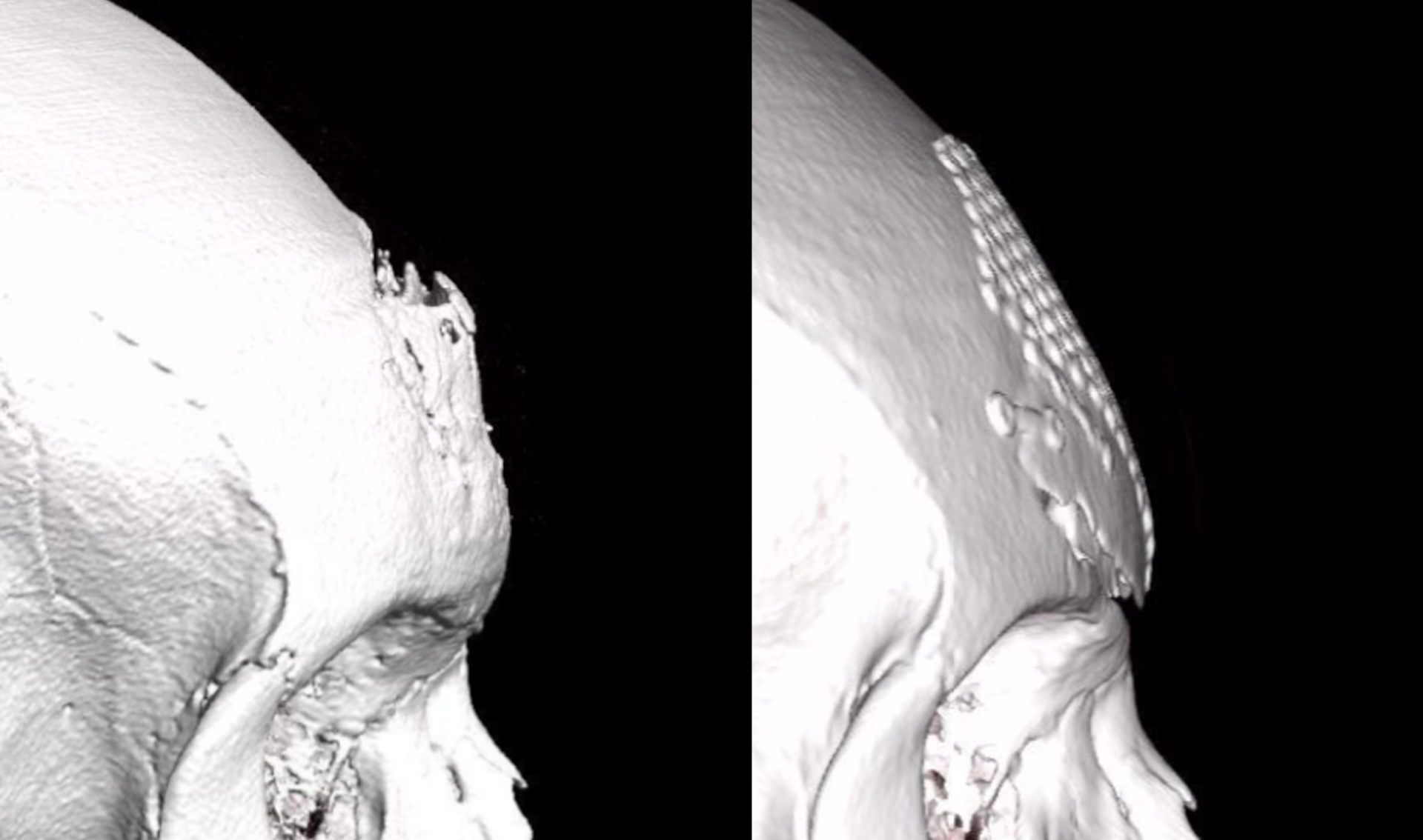
- Depressions in the sinus region. As explained above, these may appear as a consequence of excessive burring, poor fixation of the anterior wall of the sinus, etc. In this case, in addition to aesthetic problems, the patient may have associated functional problems (sinusitis, sinus blockage, visible respiration on the forehead, etc.). For that reason, in addition to correcting the aesthetic problem, we need to ensure correct functioning of the sinus, guaranteeing that it is as sealed as possible. Bone grafts and osteosynthesis material can be used (Fig.2).
- Irregularities associated with filler material. When the filler material is responsible for the problem, it must be removed and the affected area repaired (Fig.3).
- Problems related to the frontal musculature. Given that the problem does not lie in the bone plane, the treatment must focus on the muscle. When there is asymmetrical movement, botulinum toxin (Botox) can be applied to obtain correct functional compensation. If the problem lies in the volume (a partial loss of muscle volume), the defect can be corrected or camouflaged using filler material (fat or hyaluronic acid).
If you found the contents of this article interesting, we encourage you to share it. We trust that we will continue to be able to answer any questions related to facial feminization surgery that you may have in our future posts.

Hello world! I’m Lilia Koss and I use she, her, and they pronouns. What are yours? With a background in humanities and diverse professional experiences, I have been working with the Facialteam founders and directors since 2008. Involved from the ground up, so I’ve had hands in many pots: patient coordination, orientation events on 3 continents, social media, written and audiovisual content about our gender-affirming healthcare...but now life is more defined. Lately, I focus my energies on Public Relations, community management and live streaming to help raise the visibility of trans health. Life is pretty complete.